[I will add more links to relevant material as I find it.]
Transcription of BBC The Big Questions, 2nd March 2014
Nicky Campbell:Now, on Monday week, parliament will be asked to vote on whether the Secretary of State for Health should have the power to close hospitals in England even if the staff and local communities are opposed to it. It's a matter of keen interest here in Peterborough where the local hospital is in deep financial trouble. Has the time come to phase out local hospitals? Welcome to Professor Terence Stephenson, chairman of the Academy of Medical Royal Colleges. It's great to have you here.
How on earth is phasing out local hospitals putting patients first?
Professor Terence Stephenson: It's always couched as 'hospital closure' but it's hardly ever that. What the people in this audience want is the right treatment, in the right place, at the right time.
I've spent the last week, from dawn to dusk, looking after emergencies and what's preventing doctors like me giving people like this the best quality care they can is the fact that we're trying to run 20th-century hospitals in 21st-century medicine.
So there's two things we're struggling with, just two things. Two things. One is that all the evidence from strokes, trauma, cancer, heart attacks, is that if anyone in this room now is ill, the best chance of surviving that illness is somewhere where we do lots of it. And the second reason~
NC: Expertise?
TS: Expertise. You know that if you have a MFI flat-pack, you build a couple of them a year, they don't fit together, the draws don't come out. If you're doing seven- ten-a-day, you get very good at it.
NC:We're not talking furniture, we're talking people.
TS: Everybody... same principle. The more you do, the better you get. That's common sense.
Second point is that, on this Sunday morning, there will be 220 hospitals in the United Kingdom available and open for children's emergencies. About half of those, 110, in the next 24 hours will only admit six or seven children. And half of those, fifty of those hospitals, will be less than thirty minutes drive from another hospital admitting seven children. Both of them need to be fully staffed and currently we can't staff them. They'll be 30% short of Accident and Emergency consultants, 30% short of paediatricians, short of children's nurses. So we can't staff them and we need to have the volume, the expertise~
NC:So for some people, there will be a longer journey.
TS: For some people it will be a thirty minute journey.
NC: Does this make sense, Clive Peedell?
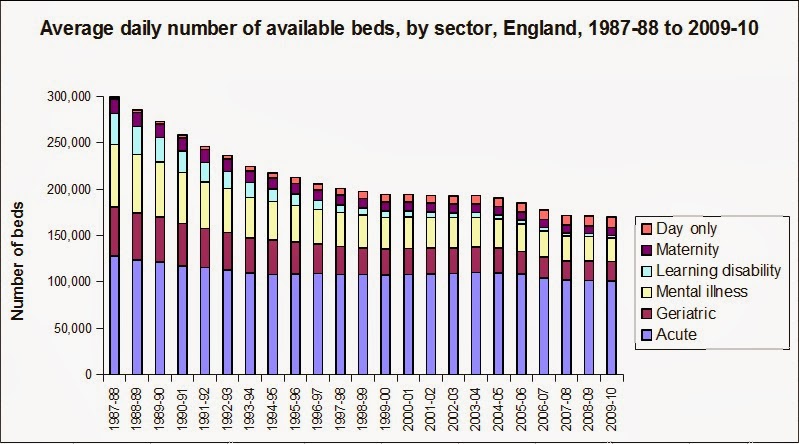
Dr. Clive Peedell: Well I think you've timed this debate very well because only in the last week in the BMJ - the British Medical Journal - there was a publication that showed that actually the number of hospitals we have compared to other countries in the OECD [Organisation for Economic Co-operation and Development] is extremely low. So we've got too few hospitals already in this country, we've already seen the number of beds cut from 300,000 to just under 150,000 in the last twenty years.
Now some of that is due to changes that need to happen, but we've got bed occupancy rates of 90% plus when the safe level is around 85%. So clinically this could be very dangerous and - [addressing Prof TS] I'll come back to your specific point about heart attacks and strokes - I agree with Professor Stephenson, there's clear evidence that centralising some services can improve survival. What those studies don't actually show is what actually happens to all the other conditions. I you close your local hospital, what happens to the acute asthmatic who has to travel a lot further? What happens to the choking child? What happens to all the other medical emergencies? That data doesn't look at that. It doesn't look at what happens to changing local healthcare~
NC:So this could be dangerous?
CP: This is dangerous. And what we've seen, this austerity that's happening at the moment, there's going to be a £30bn funding gap by 2020 for the NHS, so this is not about clinical decisions, this is about finance and there's clear evidence now that if you increase healthcare spending and education - this is from the IMF [International Monetary Fund: IMF Weighs in on Health Care Reform], from Oxford University, from Stanford University - if you increase spending, actually it stimulates economic growth, not have a negative effect, because you keep your population healthier. So we need to go completely against the austerity agenda which is damaging our health of the population~
NC:And build hospitals: more hospitals, more beds?
CP: ~so it's damaging the health of the population and we're decreasing the number of services which is going to lead to increasing privatisation and medical insurance which we're going towards. It's outrageous.
<applause>
NC: Julia Manning, this is 'outrageous', but you believe that keeping local hospitals open, they're not safe, don't you?
Dr. Julia Manning: I absolutely believe they're not safe and this is not about cutting services, this is about changing the way we deliver services so they're fit for this generation and the next generation. We still have the old model of lots of hospital services, people going to hospitals, even though most of us know that when you go to hospital, you're not in there for - you know, when you've had an operation - for a week or two. A lot of surgeries now: day surgery. We need to be using what we have in terms of resources and our people in a much more intelligent way so that we can actually meet the needs of the current population~
NC:They only fit the needs of the population if they have to travel further to visit their relatives in hospital and the relatives know that they might not be getting visits as frequently. You know, that's got to be bad for anyone who's recovering in hospital - and that might be a consequence of this.
JM: Well we need to remember that the majority of healthcare takes place in the community already and that is where the most patient-professional contacts take place, it's in primary care in the community. Hospitals are only a small part of the NHS, but we seem to have a National Hospital Service instead of a National Health Service. We need to make it fit for purpose for this century. We're not using technology in the way that we should. This nonsense that I should have to visit... go to a hospital to see a consultant to have a conversation I could have on the phone, they then tell me that I need to have tests and come back for them, tests that I could have in my GP surgery. I mean, the time wasted, we're not using technology in the way that we should, whether that's phone, Skype...
NC:Caroline Molloy?
Caroline Molloy: We hear these arguments and actually the evidence base, apart from a few selected conditions is - by the advocates' own admission - weak, and I think we need to have these sort of discussions on a case-by-case basis. You know, the public is frankly not convinced that we... I personally am sick of being patronised by experts who tell me that it's better for my health to close my local hospital. You know, and I think we need to be able to be having those discussions in our local community. We were told in the Act, 'No decision about me, without me' after all, and what they're trying to bring in with this legislation is a fast track to the procedure~
NC: So do you think this is circumventing local democracy?
CM: Absolutely, it explicitly allows no more than 40 days. I mean, as someone who has campaigned against hospital privatisation, 40 days is no time to mobilise and save your local hospital.
<applause>
NC:Let's look at the evidence in a second. I want to hear from people in the audience. Okay, I'll do that in a second, let's look at the evidence. These big centres of excellence - is there concrete, statistical evidence that they save lives? Julia Manning?
JM: When there are specialist centres yes, as Professor Stephenson said, absolutely. You want to go to a specialist centre. Now if I had a~
NC:~and lives have been saved?
JM: Absolutely. If I had a rare... if I had a rare uveal tumour in my eye, I would want to go nowhere else but the Royal Liverpool Hospital because that is where they specialise. There's no experitise in the world better than that. I would take a train to go for that~
<applause>
~We must remember the bigger picture. We have a £30bn funding gap in the next 8 years, that's just for keeping services as they are. Where do we get that money from? We either take it from other services - education? Do we really want to do that? From our communities? Or we raise taxes, but to raise taxes to raise that money, you're looking at on the average salary and extra £100 tax a month.
NC:And it's going to get a lot worse as the population gets older as well. Part of the problem here Clive, is that with these monster mortgages that the hospitals have as a result of the Private Finance Initiative. I mean, they are just frightening mortgages~
CP: We're talking about funding of the~
NC: I'm sorry, they were set in sunnier times so they came back at a rate of interest they'd never be paying back if they were set now.
CP: Absolutely. Look, Julia's right about specialist centres, but we need both. You need your specialist centres and you need your smaller hospitals as well. I'm a cancer specialist, I work in a specialist hospital, but I also do peripheral clinics in my local hospitals so I can deliver a radiotherapy service to the wider community. But you can't afford to have the equipment in every hospital, it's extremely costly and you need a lot of expertise so you need both.
Actually, we need more funding of the health service. People are saying, 'Well where are you going to get it from?' We're wasting billions of pounds on a healthcare market. We've got this purchaser-provider split with GPs buying care off hospitals, we've got a market: patients becoming 'consumers' of healthcare. That just drives up costs. It's wasting £10bn a year.
We've also nationally got huge tax avoidance problems. £70bn a year in tax avoidance. We need HMRC to stop concentrating on the small people - focus on the big people. There are thousands of people that~
<applause>
So there's huge problems and we need to settle arguments about funding because healthcare funding stimulates economic growth~
NC:~Professor Stephenson... [to audience] Get your hands ready, I'll be coming round the audience, I know this a live and important issue locally... Professor Stephenson, clamping down on tax avoidance? Is that ever going to be enough to pay for what we need in the future, going ahead with this aging population.
TS: It's not about paying. I started from it's about giving people the best quality care we can give. We lag behind countries like Sweden, Norway. [OECD national healthcare comparison study PDF] If you visit those countries, people recognise that the best quality care is not delivered by having 220 hospitals~
NC:They have far higher tax rates.
TS: They have, there are other differences, but right now... I worked in a centre for 22 years where we had no local children's heart surgery. Most of that time we didn't have adult heart surgery either. I never ever, ever heard a patient or relative say I don't want to go by aeroplane to Glasgow or Newcastle. Every single time they said, 'I want to go where I can get the best treatment possible and the best chance of surviving.'
<applause>
NC: Okay. Yes, you sir - can we get the microphone down. A very good morning. A quick point so we get through the audience.
Audience Member #1: I think we have to see this economy as a whole, because already the public-private partnership, this privatisation of hospitals is going on. We have to see that there's an argument here that there is no money here, there's a funding gap. I mean, there is money in the economy here. Just take an example of all big banks which are taking bail-outs from the government. Just last year, Royal Bank of Scotland -RBS - had £146bn in their profit and £9bn they paid out in bonuses of their executives. That's what's going on in this economy. Why can't this money be thrown into health services to fund hospitals?
<applause>
NC: You sir?
Audience Member #2: ~to the Professor here, if you were really ill and if I had cancer, we've got a great new district hospital in Peterborough, it's in financial problems mainly because of Labour's failed Private Finance Initiative, but if you had cancer in this part of the world, you'd want to go to Addenbrooke's in Cambridge which is a teaching hospital.
NC:Is that... well... we'll ask the professor about that in a second. Moving along, you sir?
Audience Member #3: I think we have to look at what's driving the proposed clause to the care bill.That was brought in by... well Jeremy Hunt has tried to insert this clause in order to give him unprecedented powers to close local hospitals~
AM#3: Yeah, in the wake of the Lewisham decision where he was deemed to have acted beyond his powers. But what we're seeing with the closures, a lot of the closures are things like Acccident & Emergency services, now just to give an example of the consequence of that: in Chase Farm, a hospital in London, they closed the Accident & Emergency service there. Weeks later, a mother rushed her young child over to Chase Farm, not realising the Accident & Emergency service had closed and as a consequence of that had to rush around and try to find another hospital, which was the increased travel distance, and there was a very tragic incident where that child very, very sadly died.
NC:Okay, just to put that point, is that a Trade Union badge by the way?
AM#3: It is.
NC: So this is something you would know about. We don't know the individual situation there Julia Manning, but are these inevitable consequences of closures?
JM: That's a tragic, tragic story and out heart goes out obviously to that mother~
NC: But are stories like that the inevitable consequence?
JM: That is a failure of publicity and telling the public what's going on with their health services and this is why this debate is so important becasue the public need to realise, not only do we have a £30bn funding gap over the next 8 years, that doesn't take into account the rising incidences of diabetes, of dementia, of sight loss. We've got to fund that as well. We cannot go on funding so many buildings and pouring money into them, we need to put the money into people and into services.
<applause>
And it is not about closure, it is about transferring and changing.
NC:Caroline?
CM: We are continually told our suspicions are wrong. We were told here in Peterborough that the Private Finance Initiative scheme wasn't unaffordable and that was conspiracy talk and then we're told a few years later that it was an absolute catastrophe and that the only answer is to sell it off and privatise it. I think our fears are grounded and they need to be heard. Where I live there is a district hospital that people have fought very hard to save, we're now being told those service, it's not the best place, you know the kind of points you're making and that we'll have community-based care in much the same way that we were told 20 years ago about mental healthcare and care in the community.
Those services simply aren't there.
District nurses numbers - who are supposed to be picking up the pieces when all these little hospitals close down - and it is about closure Julia, we've lost many... we're losing a lot of beds at the moment - and these district nurses who are supposed to be picking up the pieces, their figures have declined 40% in the last 10 years.
CN: Julia Manning?
JM: We need to change the way we train nurses. We still train nurses and doctors in hospitals, but the majority of care needs to take place in the community, so~
CM: In London, they trained five district nurses only in the last year and this is supposedly the big new hope.
JM: So why are we not looking fundamentally at the way that - not just the way that the public use services - but the way we plan them, the way we train staff. We need to make it fit for the next generation, so that my daughter has got the certainty of being able to have her children on the NHS in a place which is safe and secure, where she's going to get the best possible outcomes. That's not going to happen if we don't fundamentally change the way we deliver the majority of services.
CP: You've got to fund it.
NC: Is there evidence? [to Clive Peedell] You said there was evidence that people are dying because of closures.
CP: There is evidence from Newark hospital. The A&E closed a couple of years ago - it's subject to an ongoing investigation - but the mortality rate of people within that region, emergency admissions, has gone up by about 30%. Now that needs to be looked at to confirm, but that's just an example - because people are having to travel much further. The ambulance time, the ambulance journeys are going a lot on... Julia, we fundamentally agree about a lot of things, but it has to come with the funding and this government has a clear agenda to cut the amount of spending right across the board - not just for health services, but right across the board.
JM: That's because we don't have the money.
CP: So privatisation is inevitable. A mixed funding system: so health insurance is coming our way and I'm so angry about this I've actually co-founded a political party - the National Health Action Party.
NC:Who are you standing against?
CP: I am - this is a formal announcement today - I'm going to stand against David Cameron in Witney on an NHS ticket, for the 2015 general election~
<applause>
And the people of Witney will have the opportunity to keep the NHS if they want to, because if we carry on the way we are, we're going to lose our National Health Service.
<applause>
NC:Professor Stephenson... we've debated the privatisation issue before, right here on The Big Questions. Professor Stephenson, this leads us to the conclusion that we've heard from Clive: we're losing out National Health Service. Are we?
TS: No, it's not about privatisation, nor is it about hospital closure. Peterborough is a city with 184,000 people, it's about 39 miles from Cambridge, it's not much further from Leicester, two huge centres. If you have a condition that can be treated at home, the best place for it to be treated is at home. If you have a condition that allows you to be treated in Peterborough, sure - best to stay in Peterborough. If you have something complex that needs more technical expertise, better you go [to] some centre where they do lots of it. It's not either/or and it's feeding the public... it's misleading the public - there's hardly any example in the country where hospitals close and there's nothing. They move to a service where you have immediate, urgent care and if you're seen in a category that needs help, paramedics transfer you to somewhere that can deliver you that care.
NC:It's a difficult sell though, I mean it's quite a lot of~
TS: It is a difficult sell and politicians can't do it because~
NC: No, MPs aren't going to stand up for their constituents and say 'close our local hospital'.
TS: The MPs will be the first to say it will cost them 10,000 votes in every single el... they know that. Anne Keane's been on~
CP: That's dangerous. When someone presents with an illness, you don't know how ill they are until they've been assessed. If someone comes in with a headache, it could be meningitis, it could just be a migraine.
TS: ~so they need to see an expert to be assessed~
CP: ~If they've gone to an Urgent Care Centre, you know, where they've lost their local A&E, they would have gone to ITU [Intensive Treatment Unit], but they've no longer got an ITU, they've got an hour down the road~
NC: Wait, wait, wait. Clive, wait. Professor?
TS: They need to be seen and assessed by expert medical nursing staff and having done that, they need to be triaged. Do they stay? Stay-and-play, swoop-and-scoop. That is the modern, 21st Century healthcare. It's not about everyone doing everything in an immediate way and whilst we've been hearing about individual examples - and they are tragedies - let's not be complacent about the fact that right now, today, the outcomes, survival of people in this country today is worse than France, worse than Germany, worse than Holland, worse than many comparable countries. We want to get up to that standard of care. We won't do that by dwelling on one person. We have to look at~
CP: They've spent billions of pounds more than the NHS for decades. For decades. Decades...
NC:If we were starting again Clive Peedell, if we were starting again... (decades...)
CP: Absolutely.
NC: If we were starting again with a blank sheet of paper, wouldn't we - you - be designing a National Health Service rather like the vision that the Professor has? Julia Manning is agreeing. I thought she rather would. Local health centres dealing~
CP: The National Health Action Party has got a 12-point plan. Go and look at it. It's a publicly-funded, publicly-provided and publicly-accountable system. Which will be funded.
NC:Rather than your 12-point plan, which we'll be reading about - and I'm sure David Cameron will be going over it with a fine-tooth comb.
CP: You need to plan the system, Nicky.
NC: Caroline? We'll be starting with medical centres and big centres of expertise, wouldn't we?
CM: No-one's arguing for nothing to change, but I think it's important to remember in 2010, there were independent studies by the Commonwealth fund, by the OECD, the NHS in terms of pounds spent per life saved - and I see Terence is nodding, and Julia - was one of the most efficient systems in the whole world~
<applause>
...and that's why people are so proud of it in this country and we hear about these new technologies that can come in and have this different, more effective system - we heard this message about the 111 service - and I hear people laughing - that's a classic example: technology was rolled out, 'oh you don't need to go and clog up hospitals and block beds, just call this number...'
NC:That's an example of promises that didn't materialise.
CM: And it's happened so many times.
JM: That was not to do with technology.
NC: Last word from the audience. Terence, I'll give you the last word in a second. If I may call you Terence rather than Professor.
TS: You may.
<laughter>
NC:Yes, a quick comment if you would. That's you.
Audience Member #4: On the terms of saying that these are tragic stories, and they are really sad and can't be helped and should not be focused on too much, if I hadn't have got to hospital within 3 minutes of when I had an anaphylactic shock, I wouldn't be in this seat. So you can't just ignore the tragic stories~
JM: We're not.
AM#4: If I couldn't get to hospital, if I had an anaphylactic shock now and my next hospital was too far away, I wouldn't survive and that's the reality.
NC: What's your name?
AM#4: Ruth.
NC: Ruth. Ruth's situation - she might not be here today in our audience. This is the final word.
TS: Final word? Well, I've worked in the NHS all my life. I've never seen a private patient, despite being frequently asked becasue of my expertise. You see, I believe... I believe in the NHS, free at the point of delivery. What I'm asking for is an NHS that can deliver 21st century care comparable to other countries.
[addressing Ruth] And for you: three minutes, you want the paramedics to come to your home and if you're that ill, get there within three minutes. Don't be relying on getting somewhere else. The modern world is that the medicine comes to you, triage, and takes you to the facility that can best deliver the high quality care that will hopefully get you to survive and go home.
NC:Thank you all very much indeed. Thank you.
Now, if you have something to say about that debate, log onto bbc.co.uk/thebigquestions and follow the link where you can join in the discussion online or you can contribute on Twitter - @bbctbq